ALARA Newsletter - Issue 26 - February 2010
- Details
Author: S. Hennigor (Radiation Protection Manager, Forsmark NPP, Sweden)
The incident
In the beginning of May 2009 a contaminated car was discovered by the vehicle monitoring system at Forsmark NPP in Sweden. The inside of the luggage compartment was found to be contaminated, but there was no specific contaminated equipment or goods.
After a retrospective reconstruction of the actual use of the car it was suspected that goods, transported from RCA by the same car one week earlier could be the source of the contamination. Before the goods had been taken from RCA they had been used during construction work in a room where surface contamination may occur. The contamination emanates from the reactor coolant system. The goods, mainly consisting of some buckets, a concrete sack and tools for construction work, were tracked to a storage location outside RCA but within the NPP industrial area.
When measured by RP staff one of the buckets was identified as the main source of contamination. The contact dose rate in the bottom of the bucket was 11.5 mSv/h, emanating from small metal fragments. Also some contamination was found outside the door from RCA where the goods had been taken out, and outside and inside the store where the goods were found.
All the contaminated goods were transported to RCA and cleaned of loose contamination. Also the storage outside RCA and the outside areas were cleaned.
The total activity spread by this incident is estimated to 25 MBq, mainly corrosion products normally found in the reactor water system. About 6 MBq of the total activity had remained in the car when the contamination was discovered.
The incident was reported to the competent authority as soon as possible. It has by the NPP been judged to be outside the INES scale.

Figure 1. The contaminated car
The root cause
A root cause analysis has been performed which recommended a number of countermeasures in order to avoid this type of incident in the future.
Before removal from RCA the goods had been searched for contamination by the RP staff. No contamination was detected. However the goods were taken out from RCA one day after this check was performed and no repeated measurements were made. It is assumed that it was during this time the goods were contaminated, but it is not possible to say how. After this incident the procedures for taking goods out from the RCA have been changed and it is now only permitted to take out goods with RP staff present and immediately after the goods has been cleared to be free from contamination. Contaminated goods shall of course be treated as a transport of radioactive material when leaving RCA.
Other countermeasures that will be considered:
- Dedicated storage available within the RCA to avoid the need to take this type of material in and out.
- A special locked area inside the exit door designated for material which shall be transported out from RCA.
- Transports from RCA may only be performed at specified times.
- This kind of work shall be better planned and risk assessments shall be performed.
- The work supervisors shall be present in the actual work place to monitor work performance to a greater extent.
- Details
Authors: M. Ginjaume1, E. Carinou2, F. Vanhavere3, G. Gualdrini4, I. Clairand5, M. Sans Merce6
1 Institute of Energy Technologies, Universitat Politècnica de Catalunya (UPS), Spain
2 Greek Atomic Energy Commission (GAEC), Greece
3 Belgian Nuclear Research Centre (SCK-CEN), Belgium
4 Radiation Protection Institute - Ente per le Nuove Tecnologie LEnergia et lAmbiante (ENEA), Italy
5 Institut de Radioprotection et de Sûreté Nucléaire (IRSN), France
6 University Hospital Center Vaudois (UPC), Switzerland
The CONRAD project, funded by the EU within FP6 from 2004 to 2007, aimed to coordinate research on radiation protection in the workplace. One of the working groups in the network highlighted high extremity doses and a lack of systematic data analysis on exposures to staff in interventional radiology and nuclear medicine [1]. To improve the standards for protection of medical staff for procedures that may result in high exposures, a project called ORAMED Optimization of Radiation Protection of Medical Staff, was launched in 2008 within the framework of EURATOM FP7. ORAMED focuses on having better knowledge of extremity and eye lens exposures and developing new technologies for eye-lens measurement and for active personal dosemeters to be used in pulsed fields.
Ten Institutes, Belgian Nuclear Research Centre (Belgium), Commissariat à lEnergie Atomique (France), ENEA Radiation Protection Institute (Italy), Federal Office for Radiation Protection (Germany), Greek Atomic Energy Commission (Greece), Institute for Radiological Protection and Nuclear Safety (France), Nofer Institute of Occupational Medicine (Poland), Slovak Medical University (Slovakia), Universitat Politècnica de Catalunya (Spain), University Hospital Centre Vaudois (Switzerland) and two enterprises, MGP Instruments (France) and RADCARD (Poland), are taking part in the project. The activities are divided into 5 Work-Packages:
- optimization of radiation protection in interventional radiology,
- development of practical eye lens dosimetry in interventional radiology,
- optimization of the use of active personal dosemeters in interventional radiology,
- improvements in extremity dosimetry in nuclear medicine, with special emphasis for PET applications and nuclear medicine therapy, and
- knowledge dissemination and training.
The project is to be finished in February 2011, thus the activities are still under progress. A summary of the main objectives and activities developed until now by the different work-packages are described in this paper.
1. Optimization of radiation protection in interventional radiology
An extensive campaign of measurements and Monte Carlo calculations of extremity and eye lens doses in interventional radiology is in progress to obtain a set of standardized data on doses to staff in interventional radiology and cardiology and to design recommended radiation protection measures in order to optimize staff protection.
Figure 1 shows an image of the geometry and mathematical phantoms used for the simulation of the patient and physician during an interventional radiological procedure.
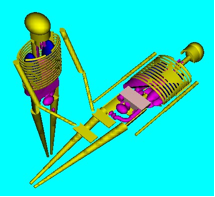
Figure 1. Mathematical phantoms and geometry used for MC simulation of interventional radiology procedures
So far, more than 660 procedures from 22 European hospitals have been analyzed. The monitored procedures are divided into three main categories: cardiac procedures; general angiography procedures; and endoscopic retrograde cholangiopancreatography procedures (ERCP). The eyes, wrists, fingers and legs of physicians are monitored and measured doses are correlated with radiological parameters such as the tube voltage and the air-kerma area product. The highest doses are often found in the left monitored finger but many parameters, such as, the availability and use of protective equipment (lead-glasses, mobile shields), tube position (above or below the table), access (femoral or radial) and a number of other procedure characteristics (use of cine/fluoro, beam projections etc) are found to influence the extremity and eye lens doses. A significant dose reduction is observed when the tube is below the table and/or when shielding is used. Finally, it should be mentioned that the examples of bad practices encountered during monitoring of the above procedures (hands inside the beam, improper use of additional protective equipment) strongly indicate the need for radiation protection training of the medical staff.
2. Development of practical eye lens dosimetry in interventional radiology
Increased evidence of radiation-related lens opacities in interventional radiologists has been reported in recent years [2]. However, the eye lens doses are never measured in routine procedures and, at the present time, there is a lack of methods to measure such doses. At the moment, a protocol to calculate and reproduce the operational quantity, personal dose equivalent at a depth of 3 mm of tissue, Hp(3,α), in calibration laboratories has been developed and a set of conversion coefficients from air kerma to Hp(3,α) has been proposed [3]. In addition, on the basis of the computed quantities, a dosemeter prototype, optimized to respond in terms of Hp(3) is under development by RADCARD. Figure 2 shows one of the prototypes. The overall procedure is also supported with type test irradiations carried out at the Laboratoire National Henri Becquerel, CEA Saclay.

Figure 2. Eye-lens dosemeter
3. Optimization of the use of active personal dosemeters in interventional radiology
Active personal dosemeters (APD) have been found to be very efficient tools to measure occupational doses in many applications of ionizing radiation. However, their use for interventional radiology cannot be generalized. The behaviour of 7 commercial APD models, deemed suitable for application in interventional radiology, has been analyzed through several tests under laboratory conditions with reference continuous and pulsed X-ray beams. Figure 3 presents a photograph of the tested APDs.


Figure 3. APDs tested in ORAMED
Most tested APDs present a satisfactory response at low photon energies, down to 24 keV, which is sufficient for interventional radiology. However, some of them do not fulfil the ISO 61526 standard requirements [4] concerning dose rate and angular response. Tests in pulsed mode show that the limitations of several APDs are mostly due to high dose-rates rather than to pulse frequency. This point was confirmed by tests in hospitals. These results have identified those devices that can provide useful indications of personal doses during interventional procedures, and those that should not be used in this field. The development of a new prototype that would overcome the present limitations of the APDs is being undertaken by MGP Instruments.
4. Improvements in extremity dosimetry in nuclear medicine, with special emphasis for PET applications and nuclear medicine therapy
Extremity doses in nuclear medicine, especially in therapy, can be very high if adequate radiation protection measures are not followed. As in the case of interventional radiology, a European campaign of extremity measurements in nuclear medicine departments is in progress. The doses to the different parts of the hands have been systematically mapped in more than 100 workers from 31 nuclear medicine departments, with special attention paid to 90Y unsealed therapy sources. Special gloves have been designed to measure the hand dose on 11 different points of the hand. Figure 4 illustrates the procedure of radiopharmaceutical administration in nuclear medicine. The technician of the photograph is wearing the ORAMED special gloves to monitor the distribution of dose in the hands.

Figure 4. Radiopharmaceutical administration in nuclear medicine
Monte Carlo simulations are simultaneously performed to determine the main parameters that influence the hand dose distribution and the effectiveness of different radiation protection measures.
Preliminary results show large variations of skin doses across the hands depending on the radionuclide and the procedure, but also large differences are found between technicians. In some cases, skin dose equivalent limit could be exceeded. The final analysis of the results should provide information on the real doses to nuclear medicine workers and help to identify the best practices in this field.
5. Knowledge dissemination and training
The training material which is being prepared within the framework of ORAMED will aim to give a practical understanding on how to improve radiation protection practice in some medical applications where, at present, doses are potentially high. The problems analyzed are, in general, not included in most available training courses for medical staff. The training material will improve actual education information. The contacts and collaboration with professional societies and international organizations should enable widespread dissemination of the material.
Along these lines, ORAMED members are involved in the recently created Medical ALARA network (EMAN), which has as main objective the establishment of a sustainable network where different stakeholders within the medical sector will have the opportunity to discuss and to exchange information on different topics related to the implementation of the ALARA principle in the medical field.
In addition, in January 2011, an international workshop to present the main results of the ORAMED project will be organized in Barcelona. Round tables with the identified stakeholders will be programmed to promote good discussion and feedback of the results. The e-learning modules will be presented on this occasion and made available to collaborating professional organizations and interested institutions in the field.
For more information, you are invited to visit the ORAMED web-site www.ORAMED-fp7.eu.
References
[1] Vanhavere, F.; Carinou, E.; Donadille, L.; Ginjaume, M.; Jankowski, J.; Rimpler, A.; Merce, M. S.; An overview on extremity dosimetry in medical applications. Radiat Prot. Dosim. 129: 350-355, 2008
[2] Vañó, E.; González, L.; Beneytez, F.; and Moreno, F. Lens injuries induced by occupational exposure in non-optimized interventional radiology laboratories. Br. J. Radiol. 71: 728-733; 1998.
[3] Mariotti, F.; Gualdrini, G. ORAMED Project. Eye-lens dosimetry. A new Monte Carlo approach to define the operational quantity Hp(3), ISSN/0393-3016, RT/2009/1/BAS.
[4] International Electrotechnical Commission. Radiation protection instrumentation. Measurement of personal dose equivalent Hp(10) and Hp(0.07) for X, gamma, neutron and beta radiation: Direct reading personal dose equivalent and/or dose equivalent rate dosemeters (1998) IEC 61526 Geneva: IEC
Acknowledgements
The research leading to these results has received funding from the European Atomic Energy Community's Seventh Framework Programme (FP7/2007-2011) under grant agreement n° 211361.
- Details
Author: Stephen Fennell (Radiological Protection Institute of Ireland - RPII)
Introduction
In 2002 Ireland submitted its national report to the meeting of the Oslo-Paris (OSPAR) ad-hoc working group on Radioactive Substances (RSC) describing how it intended to implement its strategy with regard to the discharge of radioactive substances to the marine environment. In assisting the Department of the Environment, Heritage and Local Government (DEHLG) in preparing Irelands submission to OSPAR the Radiological Protection Institute of Ireland (RPII) carried out a comprehensive review of the use of unsealed radioactive sources across all sectors throughout Ireland. The discharge of iodine-131 through patient excreta, arising as a result of activities administered to patients undergoing thyroid ablation treatments, was identified as one of the contributors to the total activity of unsealed radionuclides discharged to the marine environment from Ireland each year. In reviewing the use of unsealed radioactive sources in the medical sector the RPII determined that it would need to review its own regulatory requirements in relation to the installation of sewage holding tanks in hospitals. These tanks would take waste from the iodine ablation suites and store it for a number of weeks to allow for the decay of iodine-131 prior to discharge to the sewers. This action was subsequently included in the set of intermediate goals Ireland would take to implement the OSPAR strategy.
 Figure 1. Holding tank in a hospital in Luxembourg
Figure 1. Holding tank in a hospital in Luxembourg
Iodine Ablation Therapy in Ireland
Treatment for thyroid cancer using iodine ablation therapy is currently carried out in Ireland at four hospitals located on the east and south coasts of the country. Patients undergoing ablation therapy are administered between 3 and 7.4 GBq of iodine-131 and are kept isolated as in-patients in dedicated iodine suites for up to six days. During the course of their stay approximately 80% of the administered activity is excreted in urine. In the three hospitals located on the east coast, waste from patients goes directly to the hospitals main sewer for eventual discharge into the Irish Sea, while waste from patients based in the hospital located in the south of the country is piped to a small 1000 litre delay and decay holding tank, where it is allowed to decay on average for three weeks (approximately three half lives) before being discharged to the hospitals main sewer. When the RPII originally considered the licence applications for these facilities the licensees would have been required to undertake a risk assessment of the potential doses to critical groups such as hospital plumbers, sewer workers, sewage treatment plant workers, fishermen etc. For each of these critical groups the application was assessed against an annual dose constraint of 300 µSv/yr for non-occupationally exposed workers. In all cases the doses to these groups were considerably below the dose constraint and hence consideration of further optimisation such as the installation of holding tanks was not required by the RPII. The incorporation of a holding tank in the hospital located in the south was a decision taken locally.
Consultancy Project
In June 2007 the RPII contracted the UK consultancy firm Enviros Ltd to assist it in evaluating the need to install iodine holding tanks in both existing and future iodine ablation facilities. The evaluation reviewed existing practices in Ireland in relation to iodine-131 ablation discharges to the sewers and made recommendations for an RPII regulatory policy, based on international best practice and forecasts of future activity. As part of the contract, Enviros Ltd was tasked with undertaking an analysis of the following items:
- A summary of international advice (e.g. ICRP, IAEA, EC) on best practice in relation to iodine ablation discharges;
- A summary of current practices relating to the provision of holding tanks in a selection of other EU countries;
- A review of current practices in Ireland;
- Through discussion with relevant parties and by reviewing existing literature, provide an overview of the likely future demand for iodine ablation therapies in Ireland and any implications these would have on doses to workers and members of the public and on discharges to, and concentrations in, the environment;
- An evaluation of the merits and demerits of utilising holding tanks in an Irish context including consideration of:
- Installation: building requirements, cost, retrofitting, green field, maintenance and upkeep requirements;
- Impact on radiation doses to particular groups, including patients, medical staff, hospital maintenance staff, other staff likely to be affected and the public;
- Impact on discharges to the environment and environmental concentrations.
Findings
The final report, which is available on the RPIIs website (www.rpii.ie), provides a summary of current ablation practices throughout Ireland. It notes that in 2006 91 ablation therapies were carried out using a total of 435 GBq I-131. Through discussions with relevant staff at each facility, and the Office of the National Plan for Radiation Oncology, the authors of the report estimate that over the next 5-10 years demand for ablation therapies will increase by approximately 50%. This expected increase is in part attributed to better diagnosis and increased referrals for thyroid ablation, as well as general population increase and an overall increase in the population age.
For each facility typical doses to critical groups were calculated using models developed by the former National Radiation Protection Board (NRPB) (UK) and Environment Agency (UK) through a consideration of the amount of iodine-131 administered over the course of the year and the flow rates at the relevant sewage treatment plants. The report finds that the potentially most exposed critical group is on‑site hospital plumbers who may have to deal with a blocked sewage pipe exiting the ablation suite; in these cases the exposure arises from a one-off event rather than over the course of a year. Typical doses to plumbers dealing with such an incident are estimated to be in the range of 50-70 µSv per incident.
Other critical groups considered in the analysis include sewage workers working in man accessible pipes, workers at sewage treatment plants and coastal fishing families. After the hospital plumber the next exposed member of the public is a sewer worker who receives a dose estimated to be less than 4 µSv per year. For the projected future numbers of ablation treatments the dose to sewer workers is estimated to be less than 6 µSv per year. For all other members of the public the doses for current and projected workloads are estimated to be less than 3 µSv per year.
The report finds that there is no consistent approach to the regulation of radioactive discharges to sewers across Europe. A summary of the different practices throughout the Member States as reported in EC [1999][1] and updated as a result of consultation responses obtained during this project, is provided in Table 1. The authors point out that projected doses that are at, or close to, 10 µSv per year are generally considered to not require further reduction unless it is clear that Best Available Techniques (BAT) are not being applied. The report also notes that overall, the risk-based approach taken in Ireland to the regulation of these activities is consistent with IAEA and ICRP recommendations and is also consistent with approaches in Great Britain and Northern Ireland.
Table 1. Approaches to the management of patient excreta by EC Member States as of April 2008
| Country | Management approach | Notes | |
| Direct Discharge | Delay and Decay | ||
| Denmark | X | In Denmark there is no limit for the total activity that can be discharge (that is controlled by limits for purchase and use). However, dilution of I‑131 discharges to 0.1 MBq/l is required at the point where the hospital drain meets the municipal sewer | |
| Finland | X | Discharge limits from institutions do not apply to patient excreta that may be freely discharged to sewer as long as discharges at any one time do not exceed 100 MBq and that over the course of a year does not exceed 100 GBq. | |
| France | X | Effluents eliminated by patients in protected rooms (iodine dose > 740 MBq) are normally collected via bi-sectional toilets. Effluents from ordinary sanitary installations in the nuclear medicine unit are usually linked to a septic tank. Due to the length of time the material stays in the septic tank and the brief half-life of the radionuclides, volume activity in the collector is greatly reduced before release into the sewage network. | |
| Germany | X | All facilities required to have holding tanks installed and discharges from facilities must remain below a limit of 5 Bq/l at the point of discharge into the public waste water network. | |
| Greece | X | X | Direct discharge to sewer allowed, provided that the waste is readily dispersible in water and the maximum concentration of radioactive substances is not greater than 3.7 MBq/l. For I‑131 thyroid post-operatory therapy waste decay storage prior to discharge to sewer is required to meet this criterion. |
| Republic of Ireland | X | X | Both direct discharge to sewer and use of holding tanks are currently employed. Hospitals are authorised on activity administered not discharged. |
| Northern Ireland | X | Decay storage is used, although not a regulatory requirement. Activity concentration limit of 80 kBq/l prior to discharge to sewer. | |
| Lithuania | X | Waste is retained in holding tanks for between 30 and 60 days prior to discharge to sewer. Two tanks are used, one being filled as the other is left to decay prior to discharge. | |
| Luxembourg | X | All new treatment facilities are required to install holding tanks, with patient excreta being held for a minimum of 210 days prior to discharge. Activity concentrations of I‑131 in discharges from the holding tanks to sewer should remain below 5 Bq/l. | |
| Spain | X | X | Clearance levels are used to determine disposal routes. Where activities are above clearance levels waste should be stored for decay. |
| Sweden | X | Free release to sewer the preferred option. Decision based on direct measurements at a large hospital. External radiation exposure to sewer worker of about 2 µSv calculated on basis of 50 GBq I‑131per year direct release to sewer. | |
| The Netherland | X | Radioactive waste with radionuclides with half-lives below 100 days should be stored for up to 2 years to allow for decay. No specific mention is made of requirements for patient excreta. | |
| Great Britain | X | X | Direct discharge to sewer allowed, but sites required to demonstrate BPM and that the critical group dose constraint of 300 µSv y-1 is not exceeded. Consideration being given to use of delay tanks for new facilities undertaking treatment of large numbers of patients with I‑131. |
The authors make a number of recommendations in relation to Irelands approach for ablation waste management including:
- The benefit (on the grounds of radiological protection) of retrofitting of tanks into existing facilities is grossly disproportionate to the financial cost incurred and to the logistical issues involved. Nonetheless, appropriate work control systems should be in place to minimise any potential incidents of plumber exposure;
- Fitting of delay and decay tanks into a new facility is advantageous, particularly if only one or two facilities are established. This is particularly true where multiple ablation suites may occur in the same facility and more than one patient may be undergoing treatment at one time. However, the final requirements should be assessed on a site by site basis in line with the EC guidelines for demonstrating BAT.
- Where delay and decay tanks are installed a multi-tank vacuum system has sufficient advantages that it could represent BAT. Using such a system a factor of 500 to 1000 reduction in activity through decay is achievable. This is considered sufficient to ensure that all possible exposure scenarios would not lead to a dose of 10 µSv being exceeded.
Conclusions
Following a detailed review of the recommendations made in the Enviros report the RPII formally adopted a regulatory position on its requirements for iodine holding tanks in the context of both existing and new thyroid ablation facilities as follows:
- In the case of existing iodine ablation facilities, licensees will not be required to retro-fit iodine holding tanks.
- Licensees with existing ablation facilities will be required to undertake both on and off site monitoring to validate the assumptions and calculations used in their risk assessments when first applying for a licence for ablation therapies.
- Licence applications for new ablation facilities will continue to be assessed on a case by case basis to determine whether holding tanks are required. Each licence application must be supported by a risk assessment which estimates the likely doses that would be received by critical groups (hospital plumbers, sewer pipe workers, sewage treatment plant workers, public etc) as a result of the discharges of excreta from patients having undergone ablation therapies.
In September 2009 the Department of the Environment, Heritage and Local Government formally adopted the RPIIs regulatory position as national policy for Ireland agreeing that the RPIIs licensing requirements were consistent with Irelands commitments to OSPAR.
[1] Management of radioactive waste arising from medical establishments in the European Union. Proceedings of a Workshop, Brussels, 16-17 February 1999, EUR 19254.
- Details
"ALARA issues arising for safety and security of radiation sources and security screening devices"
Authors: P. Shaw (HPA), P. Croüail (CEPN)
Workshop background, objectives and programme
Radiation protection has always included security-related provisions (for example to prevent the unauthorised use of sources), which have contributed to the overall system of radiation safety. In recent years, however, interest in security issues has dramatically increased and the challenge is to ensure that safety and security measures are designed and implemented in an integrated manner so that security measures do not compromise safety and vice versa.
The aim of the workshop was to consider how the implementation of ALARA, in terms of planned and emergency exposure situations, involving worker and public doses, is affected by the introduction of security-related measures. In the case of new equipment and procedures, there is also the question of whether exposures arising from security screening devices can be justified and optimised. In addressing these issues, the workshop tried to consider how an optimum balance between protection, safety and security can be achieved.
As with previous workshops, half the programme time was devoted to presentations, and half to Working Group discussions and their findings. Participants had the opportunity to consider the findings of each group, contribute to discussions, and formulate the final conclusions and recommendations of the Workshop. There were 56 participants from 16 different countries, and a total of 24 oral presentations and 2 posters, arranged under the following sessions:
- Introduction and scene-setting,
- Security and safety measures,
- Planned exposure situations,
- Emergency situation management (especially due to malevolent acts),
- Justification and optimisation of doses in the use of security devices.
Two afternoon sessions were set aside for Working Group discussions, based on the following topic areas:
- Implementation of the Code of Conduct and HASS - ensuring ALARA,
- Balancing security and safety - how to achieve an optimum solution,
- Management of emergency exposure situations from an ALARA perspective,
- Justification and optimisation in the use of security devices.
On the final day, the reports from the groups were presented and discussed, and form the workshop conclusions and recommendations described later. Individual presentations (papers and slides) and the working group reports are available to download from the EAN website.
Themes and issues arising
The introductory session focused on international developments, in particular from the European Commission (e.g. HASS), IAEA (e.g. the Code of Conduct on the Safety and Security of Radioactive Sources) and from ICRP recommendations (Publications 103, 109, and 111). The first two of these have largely been implemented successfully. It was noted that many security-related documents were originally issued as stand-alone documents, but the trend now was to integrate safety and security requirements, either into the same document, or at least into comparable document structures. Further integration is envisaged through the eventual harmonisation of HASS thresholds and IAEA D-values.
The new ICRP system of exposure situations was presented, for which dose constraints (for planned exposure situations) and dose reference levels (for emergency and existing exposure situations) should be set as an upper bound on the optimisation process. The message from the workshop is that there is still much work to do in terms of implementing these recommendations in practice. For example, there are questions about when the different exposure situations apply, what the actual values of dose constraints and reference levels should be, and how to apply optimisation below these values. There is now the opportunity to provide feedback to international bodies on many of these issues, and it was suggested that EAN should help by collating comments from its members.
The 2nd session raised a number of interesting issues on the balancing of safety and security measures. Although both can be said to share a common goal protecting people from harm there is a difference in approach. Safety mostly focuses on the control of the source, whereas security is concerned with controlling the actions of (certain) people. These differences have practical implications; for example safety relies on sharing information and mutual trust, whereas security may require the opposite. The workshop contained a number of presentations on the security measures being applied to different practices. Most of these described source-related controls (e.g. physical security measures), for which there would seem to be a good synergy between safety and security, even though the approach does have to be tailored to different sectors.
In contrast, people-related controls (e.g. security checks and surveillance) were not discussed in any detail, and this may well be an area where there is more potential for conflicting requirements.
The session on planned exposure situations encompassed both normal operations (i.e. in which measures are taken to counter security threats) and the recovery of orphan sources. Examples were given of training programmes for staff involved in both these activities. Such programmes can involve large numbers of persons and require much greater resources than have traditionally been devoted to radiation safety training perhaps a reflection of the societal importance assigned to security issues.
Dose constraints for security-related staff were mentioned several times; with the consensus being that 1 mSv per year was appropriate in most cases. There was less information on dose constraints for recovery staff; further developments and exchanges of information in this area would be useful.
The same issues - staff training and dose reference levels - were raised in the 4th session in relation to emergency situation management. In this context, training is important not only for radiation protection purposes but also to ensure that the emergency response is proportionate, and that the level of risk (especially to the public) is communicated in a consistent manner. More generally, as recommended in ICRP publication 109, the national authorities should prepare plans for all type of emergency exposure situations, and relevant stakeholders should be consulted during this process. Dose reference levels for emergency responders are beginning to emerge these are within the range of values recommended by ICRP, although there are significant differences in the values being proposed in different countries. There is also an operational need for derived reference levels, in terms of dose rate and contamination levels, to help guide the optimisation process on the ground. Again, further developments and information exchange in these areas would be useful.
The final oral session considered radiation sources used for security purposes, which continue to increase in type and number. In many cases, these new practices can be managed through the normal requirements for planned exposure situations, although there are some reservations in relation to the safe use of certain types of portable equipment. Special attention was given to the introduction of X-ray security screening devices (body scanners) at airports and other locations. The consensus was that such devices must still be subject to controls, even if the dose per scan is extremely low (e.g. as is the case with backscatter scanners). Furthermore, each type of use/location should be subject to the justification principle, to prevent widespread and indiscriminate scanning of the public.
Workshop conclusions and recommendations
As mentioned above, the working group reports, containing details of the discussions, conclusions and recommendations, are available at http://www.eu-alara.net/. A brief summary of these is given below.
Implementation of the Code of Conduct and HASS ensuring ALARA
- EAN should assist in compiling feedback for the EC on the practical implementation of the HASS directive.
- Better cooperation and information exchange between EU regulatory authorities on the movement of sources between Member States is necessary.
- EC Regulation 1493/93 should be reviewed to ensure that it is consistent with IAEA guidance on import/export of radioactive sources.
Balancing security and safety - how to achieve an optimum solution
- The justification of a practice is a safety judgement, but security should be considered as an integral part of the licensing and inspection process.
- Safety and security can be integrated and made to work in practice, and both should be proportionate based on realistic assessments of the credible risks, both due to accidents and malevolent acts.
- As experience is gained, more could be done to establish harmonised international security levels and controls for different categories of sources.
Management of emergency exposure situations from an ALARA perspective
- The potential radiation exposures to different persons (responders, public, etc.) from different emergency scenarios should be assessed in order that a proportionate response, including practical protection and communication strategies, can be planned.
- Plans must be flexible. In the event of an emergency it is important for the actual radiological conditions to be assessed as soon as possible, to help direct the response and facilitate information exchange between the agencies involved.
- Training of responders is essential and, where possible, should be harmonized so as to develop a common language of protection.
Justification and optimisation in the use of security devices
- The use of ionizing radiation for security purpose should not be trivialized. Thus, even when individual doses are low, the use of security screening devices should still be subject to regulatory control, with different types of use subject to specific justification.
- Public doses should be below the 0.3 mSv/y dose constraint, with a requirement for further optimisation below this dose. In practical terms this requires much lower reference doses for individual scans, with further optimisation applied through the correct setting up, operation and quality assurance of scanning systems. To this end, draft IEC standard 62463 should be agreed and adopted.
- Where possible, persons should be informed prior to being scanned, and an alternative to x-ray scanning should be available upon request.
The next EAN Workshop, on ALARA in the Medical Sector, is planned for 7-10 of June 2011, in Norway. Details will be announced on the EAN website.